
jonetta rose barras: The intersection of COVID-19, race and class
I spent last week exploring the disturbing connection between COVID-19, race and class, and speaking with experts about how it could be broken. Doing so won’t be easy, that’s for sure.
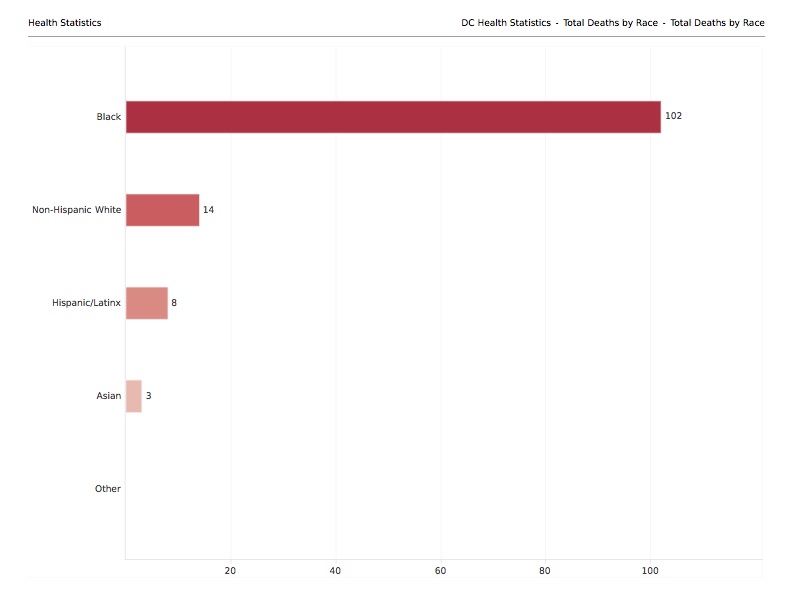
Recent statistics from New York City, Chicago, Detroit, Los Angeles and New Orleans have all revealed that a disproportionate percentage of people of color, many of them working-class, have died from the disease. In the District, 3,206 people have tested positive for the coronavirus as of April 21. Of those, 1,595 or 50% were African Americans, with race unknown for another 15%. A total of 127 people have died; 80% were black, according to data reported by the DC government. (The U.S. Census Bureau’s most recent estimates say 46.4% of DC residents are African American.)

Social distancing, mask-wearing and home confinement have constrained the spread of COVID-19. What happens, however, if there is a second wave or a new viral attack? Some researchers have suggested that more than 650,000 viral species can be transmitted from animals to humans; many of those are unknown. Does the future portend equally bad outcomes for African Americans?
No one with whom I spoke was surprised by the data. The numbers amplify weaknesses and inequities in the nation’s health care system. They also underscore historic discrimination experienced by people of color, especially African Americans, in multiple arenas — education, housing, employment, transportation, food availability, environment, and public safety. Those often combine to produce myriad vulnerabilities, including poor health.
“The institutions that failed the black community for years are now failing the entire country,” said Yesim Sayin Taylor, executive director of the D.C. Policy Center, which has consistently examined disparities affecting the local black community. “This may be an opportunity to redo those systems and create equity.”
Is it?
Is all the hand-wringing about the racial and class aspects of COVID-19 an indication that congressional representatives are ready to abandon politics and work at long last to transform socioeconomic and health care systems? Does it mean that DC officials are prepared to remodel the decades-old DC Healthcare Alliance, incorporating more aggressive preventive services? Will that $370 million hospital proposed for Ward 8 ensure equity and fewer deaths?
It “would go a long way in helping African Americans in that ward who function with tremendous health care issues,” said Wayne Turnage, DC deputy mayor for health and human services. While the current economic problems brought on by the pandemic might raise concerns about whether the city can now afford to construct or expand health care services, Turnage said that the “beauty of the deal” being negotiated with the support of Mayor Muriel Bowser is that most costs would be borne by the hospital operator.
Turnage boasts that DC has improved health care services in recent years. It is “top-rated in the country for hospital use” and “it’s ranked No. 2 for physicians and primary care specialty compared with other jurisdictions.
“However, there is a problem: It’s a tale of two cities,” he continued. “We have a well-funded, expertly stamped operation that serves with ease residents in wards 1 through 6.
“In Ward 7 and 8, there is a complete absence of a system,” added Turnage.
A new hospital is nice, but it’s a partial response to a complex problem. After all, there was a time when United Medical Center (UMC), the current hospital east of the Anacostia River, was shiny and bright, said former Ward 8 Council member LaRuby May. A series of management problems and deliberate underfunding have cast aspersion on its operation and services.
“No one sends patients to UMC: not Charter, not AmeriHealth, not Unity. We essentially are a walk-up hospital,” continued May, who chairs UMC’s board of trustees.
“We consistently treat people who have infectious diseases,” said May, noting that some of the same doctors who work out of George Washington University Medical Faculty Associates also work at UMC.
Establishing a truly holistic solution to health disparities in the country or in DC won’t be easy. It requires altering decades of cultural beliefs and behaviors by African Americans that have sometimes led to them neglecting their health or failing to proactively seek the care they need.
Consider as amplification of that fact a story Turnage told me: More than a decade ago, as a member of Virginia Gov. Mark Warner’s cabinet, Turnage was attending an event and standing next to the CEO of the Virginia Commonwealth University Hospital, Sheldon Retchin. “He asked me who was my primary care physician. I said I didn’t have one.”
Turnage hadn’t seen a primary care physician since he left high school. Retchin was shocked and referred him to the hospital’s medical director, who conducted a physical.
“I was pre-diabetic. I had hypertension. And I had high cholesterol,” Turnage explained. “I am convinced had I not done that [then], I would be dead by now.”
Many blacks in DC don’t have primary doctors, said May, who has received several phone calls from Ward 8 residents asking about being tested for the coronavirus. “I tell them they have to consult their primary physician. The majority don’t have one.”
How is that possible? The DC Healthcare Alliance program is supposed to guarantee all enrollees have a primary care physician.
May also said that many children east of the river see doctors at the branch of the Children’s National Hospital located there. But “when parents take their children to the pediatrician, they see a different pediatrician each time,” undermining the value of a regular doctor.
Unpredictable, irregular and impersonal services have exacerbated African Americans’ tendencies to be dismissive and casual toward their health care. It also has reinforced a palpable distrust of the medical profession that tracks back to reports of African Americans being used as guinea pigs. Consider the Tuskegee Study of Untreated Syphilis in the Negro Male conducted from 1932 to 1972; denied treatment even after the discovery of penicillin, some of the participants either died, turned blind or went crazy.
“Poor folks have a valid reason to distrust the medical profession,” said May. “We believe, as is true, the health care system is [largely] another white institution.”
Most experts have pointed out that COVID-19 isn’t discriminatory — it can affect everyone. After all, the first reported cases in the country were in Washington State and California. Tens of thousands of people in Europe have died from the disease. The local data in DC also amplifies the virus’s expansive reach: As of April 21 in DC, wards 2 and 3 each accounted for just 7% of the city’s confirmed cases. Wards 1 and 6 were the next lowest with 11% and 12%, respectively. The largest percentages of positive cases were in wards 4, 5, 7 and 8 — 17%, 13%, 15% and 14%. The other 3% were not connected to any geographic area.
African Americans seem to be wearing a bull’s-eye, however. Chronic diseases such as diabetes and high blood pressure that affect many of them — including middle-class folks like Turnage — make them the “perfect petri dish” for a disease that is opportunistic and relentless in its search for a host body unable to offer resistance. If you contract the virus with a severe underlying condition, “you are likely to end up on a ventilator. If you end up on a ventilator, you are more likely to die,” added Turnage.
In cities such as DC, working-class blacks, including bus drivers, janitors, garbage collectors, farmworkers, waitstaff, grocery store cashiers and stock clerks, seem the hardest hit. Interestingly, with the advent of the virus, they have been deemed essential — although they have never been paid as if they were critical to the economy.
I wonder whether playwright Douglas Turner Ward, founder of the Negro Ensemble Company, is shocked by the public adulation those workers have been receiving. His 1965 play Day of Absence explores what might happen if blacks in a Southern town disappeared, leaving whites to fend for themselves.
In the middle of a crisis, it’s easy for everyone to join hands. It’s a form of self-preservation. What happens after a COVID-19 vaccine is distributed? How many people will stand with working-class people of color? How many will demand more from the federal government than a miserly $1,200 check? How many will push for an effective, nondiscriminatory national health care system?
These are long-standing problems, but we must recognize that there are long-, medium- and short-term solutions. There’s no reason for DC officials to wait until a new hospital is constructed. In the interim, they can invest in UMC, redirecting more residents to that facility, ensuring a continuum of care.
Additionally, Taylor said the city could use other institutions, like CVS stores and school clinics, to improve access to quality health care. Existing government-funded clinics scream for improvements. “They are not operating the way they used to, when you could just walk in,” she added.
There could be a greater reliance on nurses for a more personal and personalized approach that doesn’t just force patients to “see physicians for three minutes.” And, there must be “access to gyms and good food. These issues become really important,” continued Taylor, adding that an enhanced economic environment is also critical to improved health outcomes.
“We [also] have to educate people how to use the health care system,” said Turnage, who offered as justification for greater investment this breathtaking statistic: “A child born today in Ward 7 and 8 lives 15 years less than a child born anywhere else in the city.”
That reality is not affected by the presence of COVID-19 or any unknown virus.
jonetta rose barras is an author and freelance journalist, covering national and local issues including politics, childhood trauma, public education, economic development and urban public policies. She can be reached at thebarrasreport@gmail.com.
Very informative. great Job